Geoff Cotter
Edited by Ana-Maria Oproescu
This summary was updated in 2022 by Cally Yeung, with edits by Crystal Han. The updates are shown in blue.
This is a summary of a research study conducted by ICORD Principal Investigator Dr. Kathleen Martin Ginis, Dr. Christopher West, Dr. John Steeves and colleagues. To read the original paper, please click here.
Why are exercise guidelines specific for adults with spinal cord injury (SCI) necessary?
Physical activity guidelines describe the frequency, intensity, duration, and type of exercise necessary to produce certain health outcomes. The authors of this study note the increasing public awareness of the importance of physical activity, as well as the increasing number of recommended physical activity guidelines. The authors also recognize, however, that guidelines like the one put out by the World Health Organization (WHO), recommending 150 min/week of moderate intensity aerobic activity and strength training twice a week, do not consider the complications, feasibility, and how requirements might differ for those with SCI. For this reason, the authors of this study set out to review existing research to create evidence-based exercise guidelines for improving cardiorespiratory health (cardiorespiratory fitness, power output and muscular strength), and cardiometabolic health (body composition and cardiovascular risk factors as they relate to metabolic and cardiovascular diseases) which are specifically designed for those with SCI. This study re-evaluated the Appraisal of Guidelines, Research and Evaluation (AGREE) II reporting criteria and a new scientific evidence base to create an updated guideline on the minimum and type of physical activity to improve the fitness and cardiometabolic health of adults with SCI.
The Guidelines
The guidelines produced by the authors are based on an extensive review of current scientific evidence, consultation with experts in the field and other stakeholders, and formed according to the highest possible confidence standard in their effectiveness based on existing scientific evidence.
How was the study done?
The study consisted of four researchers with expertise in physical activity and SCI, and the project involved several steps, in the following order:
- Determining the guideline parameters
- Reviewing relevant literature
- Holding three panels (European, Canadian, International) with participants to form the guidelines
- Obtaining participant feedback
- Finally, formally reviewing the guideline development process with an AGREE II expert.
Participants (87% women) were from 14 countries, and consisted of people living with SCI, health care providers, SCI community service providers, and exercise professionals.
Who are these guidelines applicable to?
As a result of their evidence base, the guidelines are not intended to inform activity for people who are not represented in the research. In this particular case, the guidelines may be appropriate for those over 65 years of age and those with acute SCIs, however these groups are not well enough represented in the research body currently for the authors to conclude that the exercise guidelines will also be optimal for these populations.
Why are there two separate guidelines?
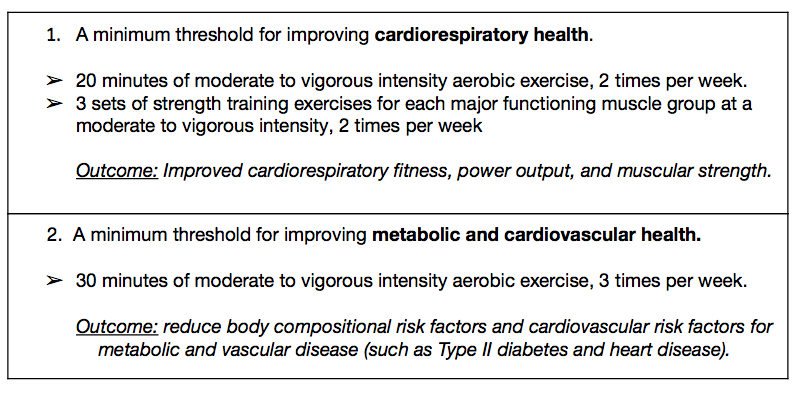
The authors note that SCI-specific cardiorespiratory exercise guidelines have existed since 2011. However, at that time there was not enough evidence to state their impact on cardiometabolic health specifically. Recently, enough new research has accumulated to allow researchers to create guidelines outlining the minimum exercise threshold at which one can expect to improve cardiometabolic health outcomes. Thus, the authors of this study approached this with a focus on ‘exercise’ (ie: planned, structured and repetitive physical activity performed to improve and maintain fitness) rather than ‘PA’ (physical activity, ie: bodily movement produced by muscles requiring the use of energy). With there still being limited evidence for cardiometabolic outcomes, the authors recognized that separate minimum thresholds for producing positive cardiorespiratory outcomes and positive cardiometabolic outcomes were necessary to recommend both with the greatest amount of confidence in each. A a result, the authors have provided two separate guidelines, one as a minimum for improving general fitness and strength, and the other as a minimum for improving cardiometabolic health.
Both guidelines developed by the authors advised lower frequency and duration of aerobic exercise in comparison the WHO PA guidelines for the general population (150min/week). This difference reflects the consideration of evidence of effective minimal dose exercise as previously backed by SCI-specific studies, instead of the optimal amount of physical activity based on evidence of able-bodied individuals. Therefore, by following new guidelines of relatively smaller doses of exercise, individuals with SCI can experience improvements of fitness and cardiometabolic health without the risk of injury from excessive exercise.
Important considerations and limitations:
The evidence available supports the guidelines’ efficacy for the following:
- Ages 18-64
- Chronic SCI (longer than 12 months)
- C3 vertebrae injury and below
- Irrespective of race and sex
The authors caution that:
- The guidelines are intended as a minimum for achieving health improvements. Exceeding guidelines may increase improvements and may increase risks, however, the authors found insufficient data to comment with certainty.
- As exercise guidelines, they are intended to inform activity beyond the activities of daily living.
- Before beginning an exercise program, consultation with a health professional knowledgeable in exercise options available and appropriate for those with SCI can help mitigate risks and inform activity options.
- Those with a cervical or high thoracic injury should be aware of the symptoms of autonomic dysreflexia before beginning.
- Those new to structured exercise should begin slowly and gradually work toward the guideline minimums.
Which guidelines should I use?
Between the two separate exercise guidelines presented in this paper and the many existing guidelines like that of the WHO, it may be confusing which guidelines to follow. The authors stress the importance of consulting a health and fitness professional who is experienced with physical activity for those with an SCI as a way of determining which outcome is most beneficial for an individual, which guideline is most feasible, and which guideline may be most relevant. For those with an SCI these guidelines should instill greater confidence in their effectiveness to produce the desired outcome given their basis in SCI research and process outlined below.
What does it mean to be evidenced-based?
The guidelines presented in this paper are evidence-based meaning they are the product of an extremely rigorous process which first involved the systematic review of relevant scientific information, assessing 211 studies in total. Extensive consultation with scientists, experts in exercise and SCI, and stakeholders helped to produce the guidelines according to the highest possible standards and confidence in the resulting recommendations. The authors concluded the process with feedback from various stakeholders in the SCI community. The authors recommend the continued reassessment of the guidelines to assure their accuracy with current research.
Definitions:
Aspects of Exercise guidelines:
frequency – how often one exercises (2 or 3 times per week)
intensity – effort involved in exercise (light, moderate, vigorous)
duration – how long an individual exercise session lasts (20 minutes)
type – general categories of exercise (aerobic vs strength training) or more specific (hang cycling vs rowing machine or free weight vs cable machine)
Cardiometabolic health – Encompasses Body Composition (various measures of fat mass and muscle mass) and Cardiovascular Risk Factors (Measures representing lipid profile, glucose levels, cardiac function, vascular structure function, inflammatory status and immune system homeostasis) for cardiovascular diseases like type II diabetes and heart disease.
Cardiorespiratory health – Encompasses cardiorespiratory fitness (exercise capacity), power output (ability to produce force quickly), and muscle strength (ability to produce muscular force)
Physical Activity vs Exercise:
Exercise is planned, structured, and repetitive activity intended for the improvement of health and fitness
Physical Activity includes any activity that involves large physical movements. ADLs and exercise.
Activities of Daily Living (ADLs) – movement and physical activity which is required to perform the necessary tasks of sustaining life. Getting dressed, eating, bathing, transferring, etc.
Stakeholders – people with SCIs, organizations involved in assisting people with SCIs, health care providers involved with those with SCIs, as well as experts and researchers in SCIs